How to Calculate EDD Formula – Predict Your Baby’s Arrival
Understanding how to calculate EDD formula is essential across multiple fields — from obstetrics where EDD means Estimated Due Date, to public policy where EDD acronyms appear in economic or employment development contexts. This long-form article focuses primarily on the clinical calculation of Estimated Due Date (EDD) — the set of methods that clinicians, midwives and expectant parents use to estimate the likely date of delivery — while placing that calculation in a wider social and policy context (maternal health planning, state-level maternal services, rural outreach, and women’s empowerment initiatives). You’ll get history, objectives, step-by-step methods for how to calculate EDD formula, comparisons with alternative approaches, implementation and measurement issues at the state level, success stories, major challenges, and future prospects.
Note: In this article “EDD” will generally mean Estimated Due Date (pregnancy). When the context switches to Employment or Economic Development (also commonly abbreviated EDD), the text will explicitly say so.
Why the question “how to calculate EDD formula” matters
Estimating a baby’s due date is not a trivial calendar exercise. The EDD drives prenatal scheduling, screening timetables (like prenatal labs, glucose testing, group B strep screening), hospital resource planning, maternal nutrition counseling, and public health programs targeting perinatal care. Errors in EDD can lead to premature induction, mis-timed interventions, or missed opportunities for antenatal care. As such, knowing how to calculate EDD formula correctly — and which method to trust in each context — is central to maternal and neonatal outcomes. Authoritative clinical guidelines (e.g., ACOG) still recommend using a combination of patient history and first- or early-second trimester ultrasound to determine the best EDD. ACOG+1
A concise definition: what “EDD” means in obstetrics
In obstetrics, EDD (Estimated Due Date) is the clinician’s best estimate of when spontaneous labor will most likely begin — conventionally 280 days (40 weeks) from the first day of the last menstrual period (LMP) in a standard 28-day cycle. Determining the EDD helps sequence prenatal care and informs clinical decision-making near term. Traditional rules (e.g., Naegele’s Rule) date back to 19th-century practice; modern methods incorporate ultrasound measures and sometimes algorithms that correct for cycle length or conception records. ACOG+1
A short history of EDD estimation and the “EDD formula”
The practice of estimating a due date has evolved:
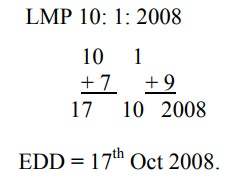
- Classical method: Naegele’s Rule (attributed to Franz Naegele, early 1800s) — add 280 days (or add 7 days and subtract 3 months from the first day of LMP). This is the classic “EDD formula” taught in many clinical settings because it approximates 40 weeks of gestation for a 28-day cycle. ACOG+1
- Ultrasound introduction: In the mid-20th century, ultrasound measurements (especially crown-rump length in early pregnancy) provided a more objective method to estimate gestational age and EDD, reducing error where LMP is uncertain. Professional bodies now recommend reconciling LMP and early ultrasound to set a single best EDD. MDCalc+1
- Contemporary refinements: Clinicians now use formulaic adjustments for irregular cycles, conception dates, assisted reproduction records, and biometric models. Digital calculators and EHR tools have embedded these formulas into workflow. UpToDate+1
Objectives: What a correct EDD calculation should deliver
When you learn how to calculate EDD formula, the objective is not only to produce a calendar date but to:
- Provide a clinically useful anchor for timing prenatal interventions.
- Minimize the risk of unnecessary early induction or missed late-term care.
- Support health system resource planning (bed capacity, neonatal services).
- Inform public health programs and outreach — especially in rural and underserved populations.
- Help pregnant people plan (work, family, transport) and access maternal support services.
A good EDD process balances simplicity (usable by clinicians and patients) with accuracy (reduces misclassification of preterm or post-term births).
Core methods: Step-by-step instructions for “how to calculate EDD formula”
Below are the primary methods used worldwide. Each method is accompanied by a clear step-by-step calculation.
1) Naegele’s Rule — the classic EDD formula
Naegele’s Rule is the foundational clinical formula for estimating due date.
How to calculate EDD formula using Naegele’s Rule:
- Start with the first day of the last menstrual period (LMP).
- Subtract 3 calendar months.
- Add 1 year and 7 days (or simply add 280 days).
Example: If LMP = September 9, 2024:
- Subtract 3 months → June 9, 2024.
- Add 1 year and 7 days → June 16, 2025. (or add 280 days to Sept 9, 2024 = June 16, 2025).
Naegele’s Rule assumes a 28-day cycle with ovulation on day 14; it is quick and commonly used in non-complex settings. However, it becomes less accurate with irregular cycles or uncertain LMP recall. Johns Hopkins Medicine+1
2) Add 280 days directly — alternate presentation of the EDD formula
A simple arithmetic variant of Naegele’s Rule:
- EDD = LMP date + 280 days.
Clinically identical when cycle length = 28 days, but easier to compute with calendar tools or software.
3) Ultrasound-based EDD (biometric formula)
When LMP is unknown or cycles are irregular, early ultrasound is more reliable. The most common early measurement is crown-rump length (CRL), measured in the first trimester.
How to calculate EDD formula with CRL:
- Perform a first-trimester ultrasound and measure CRL (in millimeters).
- Use validated charts or built-in calculator functions to convert CRL to gestational age.
- Subtract the gestational age (in days) from the date of the scan to determine conception-equivalent date; add 280 days to the LMP-equivalent date to set EDD.
Modern ultrasound machines and obstetric calculators already implement the formulaic conversions; clinicians should prefer ultrasound EDDs when discrepancy with LMP exceeds preset thresholds. MDCalc+1
4) Conception-date approach (dating from ovulation or assisted reproduction)
If the exact date of conception or embryo transfer is known (e.g., IVF), EDD is calculated directly:
- Natural conception approximate: Conception date + 266 days ≈ EDD (since conception occurs about 14 days after LMP in 28-day cycle).
- IVF/ET: EDD = Date of embryo transfer + days to reach 40-week gestation (standardized in IVF protocols).
This method is precise when conception/transfer dates are documented. Perinatology
5) Alternate formulas & corrections for cycle length
Clinicians sometimes apply cycle-length corrections when the patient’s menstrual cycle deviates from 28 days. A common correction:
- Adjusted EDD = LMP + 280 days + (cycle length − 28 days)
If a patient has a 32-day cycle, add 4 days to the naive Naegele EDD; if 24-day cycle, subtract 4 days. This approximates later ovulation timing.
Which method should you choose?
Clinically:
- If LMP is well known and cycle is regular, Naegele’s Rule (or the +280 days method) is acceptable.
- If LMP is uncertain or cycles are irregular, rely on first-trimester ultrasound for EDD.
- If conception or embryo transfer is known, base EDD on that date.
- Reconcile LMP and ultrasound: often clinicians will adopt the ultrasound EDD if the difference with LMP exceeds a guideline threshold (commonly ~7–10 days in first trimester, larger thresholds in second trimester). ACOG
From a public-health planning perspective: standardized adoption of ultrasound-derived EDDs can reduce misclassification of preterm births in a registry and improve resource allocation.
Precision, bias, and pitfalls in EDD calculation
Understanding sources of error is critical when you study how to calculate EDD formula:
- LMP recall errors: Many patients cannot accurately remember exact LMP; recall bias causes systematic error.
- Irregular cycles: Standard EDD formula assumes a 28-day cycle; variations in cycle length shift the ovulation window.
- Late presentation: If prenatal care begins late, early ultrasound opportunities are missed and dating becomes less accurate.
- Population differences: Ethnic, nutritional, and environmental differences can slightly alter average gestational lengths.
- Device and operator variability: Ultrasound measurement depends on equipment, operator skill, and fetal position.
Because correct dating affects policy (e.g., preterm birth rates), researchers and program managers should explicitly state which EDD formula they used when reporting maternal-newborn indicators.
Integrating EDD calculation into health systems and policy frameworks
Knowing how to calculate EDD formula correctly is not only clinical; it is an administrative and policy issue. Accurate EDDs enable:
- State-level perinatal surveillance: Correct dating reduces false high rates of preterm delivery that can distort program evaluation.
- Targeted antenatal outreach: EDDs let programs prioritize late-third trimester visits, childbirth education, and transport arrangements for remote expectant mothers.
- Resource allocation: Hospitals and regional health authorities plan staffing and neonatal intensive care beds around expected delivery loads.
- Maternal benefits timing: Social welfare programs that disburse pre- or post-natal support can align benefits with EDD windows.
When designing maternal health policy, agencies should require standard documentation of dating method — e.g., LMP vs early ultrasound vs documented conception — so that administrative databases are comparable between regions and over time. ACOG
State-level impact and implementation: making EDD useful for public programs
At state and provincial levels, the implementation of a consistent EDD formula practice can have measurable benefits:
- Uniform reporting: Mandating early ultrasound where feasible (or a minimum standardized LMP documentation) reduces variability in maternal-neonatal metrics across counties.
- Program targeting: States with rural populations can use EDD information to deploy mobile antenatal clinics and plan emergency transport around expected delivery clusters.
- Insurance and benefits: EDD documentation supports eligibility and timing for maternity leave, cash transfers, nutritional supplements, and conditional cash programs aimed at maternal health.
- Data-driven policy: Accurate EDDs feed into better estimates of preterm birth rates, neonatal morbidity benchmarks, and maternal mortality audits.
Case example: a state that standardizes early ultrasound dating in high-volume centers and calibrates registries to ultrasound dates often reports a lower, more reliable preterm birth proportion — helping them target neonatal intensive care scaling more precisely.
Women’s empowerment, rural development, and EDD calculation
There is a natural link between precise EDD calculation and broader developmental priorities:
- Women’s empowerment: When pregnant individuals are given accurate EDDs, they can better plan maternity leave, childcare, and vocational transitions — a component of economic agency.
- Access to care: Accurate dating that triggers timely antenatal interventions reduces adverse outcomes, which supports women’s capacity to participate in education and the workforce postpartum.
- Rural development: In remote areas, knowing the EDD lets community health workers synchronize transport, birthing center readiness, and temporary housing arrangements near referral hospitals.
- Social welfare initiatives: Conditional cash transfers, food support, and targeted maternal health nutrition programs rely on valid EDD documentation to target the right trimester for interventions.
Thus, training frontline health workers in practical EDD calculation and documentation is a relatively low-cost investment with outsized returns for maternal health equity.
Comparing the EDD formula with other maternal-health calculations
When asking how to calculate EDD formula, it helps to contrast EDD with related metrics:
- Gestational age (GA): EDD is a projection; GA is the current age of the fetus (e.g., 24+3 weeks). GA is derived from EDD or directly from ultrasound measures.
- Post-term & preterm thresholds: EDD allows classification of births as preterm (<37 weeks), term (37–41+6 weeks), or post-term (≥42 weeks) — designations that drive care decisions.
- Corrected age (for growth charts): Postnatal infant growth monitoring often adjusts for gestational age at birth; accurate EDDs thus influence pediatric follow-up.
Accurate implementation of EDD reduces misclassification across these related indicators, improving clinical and public reporting fidelity.
Success stories: when accurate EDD calculation changed outcomes
Several programmatic examples illustrate the impact of accurate EDD practices:
- Urban hospital networks that enforced early first-trimester ultrasound for all prenatal patients reduced induction for “post-dates” that resulted from erroneous LMPs — saving costs and avoiding unnecessary interventions.
- Rural outreach programs that used EDD to schedule mobile birthing units and transport plans saw reduced emergency transfer times and improved rates of facility births.
- State data initiatives that standardized ultrasound-based dating observed clearer trends in preterm birth rates, enabling targeted neonatal resource deployment.
These successes underscore the practical benefits of investing in training, portable ultrasound access, and EHR fields that capture both LMP and the dating method.
Challenges and limitations: practical barriers to accurate EDD calculation
Despite clear benefits, real-world obstacles exist:
- Limited access to early ultrasound: In low-resource and rural settings, lack of early imaging reduces the ability to compute ultrasound-based EDDs.
- Record fragmentation: When prenatal care is fragmented across providers, EDD information may be inconsistent.
- Cultural and literacy factors: Some patients may not track menstrual cycles or may use lunar calendars, complicating LMP-based calculations.
- Cost and training: Deploying portable ultrasound and training midwives or community health workers requires sustained investment.
- Administrative inertia: Health systems with entrenched reporting practices may be slow to shift to ultrasound-preferred EDDs.
Addressing these challenges requires a combination of policy commitment, budget allocation, and capacity building.
Practical recommendations for clinical teams and program managers
If you are implementing or refining EDD practices, the following steps synthesize best practice:
- Document the dating method: Capture whether the EDD is based on LMP, first-trimester ultrasound, conception/IVF date, or a corrected formula.
- Prefer early ultrasound when available: Use CRL in the first trimester as the most objective method when LMP is uncertain. MDCalc
- Use Naegele’s Rule when appropriate: For patients with a reliable LMP and regular cycles, Naegele’s Rule or +280 days remains a simple, valid approach. Healthline
- Apply cycle-length corrections if the patient’s cycle length is known and consistently different from 28 days.
- Ensure EHR fields capture both the EDD calendar date and the method used; this supports audits, research, and policy decisions.
- Build tele-ultrasound or point-of-care ultrasound (POCUS) capacity for rural clinics to improve early dating accuracy.
- Educate patients about the importance of early prenatal visits and keeping track of menstrual dates.
Technology, innovation, and the future of EDD calculation
Looking forward, how to calculate EDD formula will be influenced by technological and methodological advances:
- AI-enabled prediction: Algorithms that integrate LMP, cycle history, biometric ultrasound, hormonal markers, and wearable physiologic data may deliver refined EDD predictions and individualized uncertainty ranges.
- Wearable ovulation detection: Broader adoption of ovulation-tracking wearables could give more precise conception windows for those who use fertility tracking tools. This data could feed EHRs (with consent) to sharpen EDDs.
- Telemedicine and POCUS: Widespread portable ultrasound and remote interpretation may democratize early ultrasound dating in low-resource settings.
- Standardized reporting frameworks: International consensus on dating documentation (e.g., always recording LMP, ultrasound date, CRL, and chosen EDD) will improve cross-region comparisons.
These innovations will also raise privacy, consent, and equity considerations that policy must address.
How to communicate the EDD to patients: language, expectation management, and documentation
Clinicians must communicate EDD clearly to expectant parents:
- Explain that EDD is an estimate, not a guarantee.
- Give a gestational age range: most births occur between 37 and 42 weeks.
- Document the method used and, where applicable, explain why the EDD may be revised (e.g., new ultrasound).
- Use the EDD to time education (e.g., childbirth classes at 30–36 weeks) and to arrange practical supports (transport, leave).
Patient-centered communication reduces anxiety and supports preparedness.
Cross-sectoral link: when EDD means Employment/Economic Development Department
Outside obstetrics, “EDD” is commonly used for Employment Development Department or Economic Development Districts/Departments. In that context, how to calculate EDD formula might mean formulas used to compute unemployment insurance benefits, formula allocations, or economic indicators. For example, the California EDD provides unemployment benefit calculators and detailed formulas for computing weekly benefit amounts and program formula allocations; these are administrative formulas rather than obstetric dating formulas. When policymakers use the acronym EDD in program finance, clarity about definitions and documentation is equally crucial. Employment Development Department+1
Ethical, equity, and data governance considerations
As EDD calculation becomes more data-driven, consider these principles:
- Equity of access: Ensure rural and underserved populations can get early ultrasound or validated alternative dating tools.
- Transparency: Public health reports should specify the dating method to avoid misleading comparisons.
- Consent and privacy: For wearable or app-derived conception data, secure consent and data protection.
- Cultural competence: Respect local practices in menstrual tracking while providing clear explanation of how EDDs are computed.
By addressing these issues, programs can increase trust and uptake of maternal services.
Checklist: immediate actions for clinics and health managers
- Train staff on Naegele’s Rule and cycle-length adjustments.
- Standardize EHR fields: LMP, dating method, ultrasound CRL, date of scan, and final chosen EDD.
- Advocate for early ultrasound access in your network.
- Educate patients on LMP tracking and the provisional nature of EDD.
- For policy teams: require method documentation in perinatal data submissions.
Frequently Asked Questions (FAQs)
- How accurate is the EDD formula based on Naegele’s Rule?
Naegele’s Rule provides a useful initial estimate but is most accurate for patients with a regular 28-day menstrual cycle. Typical error can be ±1–2 weeks depending on cycle variability and recall accuracy. First-trimester ultrasound tends to be more precise. Healthline+1 - When should the EDD be revised?
An EDD may be revised if an early ultrasound (preferably in the first trimester) provides a gestational age that differs from LMP-based dating beyond accepted thresholds (often ~7–10 days). Revisions should be documented and communicated clearly to the patient. ACOG - If I don’t know my LMP, how can I calculate EDD?
Without LMP, use early ultrasound measurements (CRL) or documented conception/IVF dates. If neither is available, later ultrasound estimations can be used with caution but have larger uncertainties. MDCalc - Does the EDD formula change for multiple pregnancies?
The EDD calculation method is the same, but multiple pregnancies often have different growth patterns; clinicians may rely more on ultrasound and tailored fetal assessments. Document method and any adjustments. MDCalc - Can wearable fertility trackers help with EDD?
Wearables that reliably detect ovulation can narrow the conception window and improve estimated dating if users consent to integrate that data into clinical records. However, validation, data privacy, and standardization remain important considerations. - What’s the difference between Estimated Due Date and Expected Date of Confinement (EDC)?
They are synonyms — both refer to the best clinical estimate for the date of spontaneous labor. Historically “EDC” (expected date of confinement) was used; “EDD” (estimated due date) is the more modern and neutral term. MedComic
Final thoughts: practice, policy, and the human side of EDD
Understanding how to calculate EDD formula is much more than learning a calendar trick. It’s about creating reliable clinical anchors, enabling better maternal and neonatal care, optimizing state and facility planning, and empowering pregnant people to make informed decisions. Whether you are a clinician applying Naegele’s Rule at a bedside, a midwife coordinating transport in a remote catchment, or a policy manager designing maternal benefit windows, the choices you make about EDD calculation matter.
Practical improvements — early ultrasound access, standardized documentation, EHR capture of the dating method, and community education — are achievable steps with meaningful returns. Technological advances promise better precision, but the foundation remains: transparent methods, consistent documentation, and patient-centered communication. That is the best answer to the question how to calculate EDD formula in 2025 — a blend of time-tested rules, objective measurement, and systems that use the date wisely for health, planning, and equity. ACOG+2MDCalc+2
If you’d like, I can:
- Produce a printable clinic one-page EDD calculation flowchart (LMP → Naegele → ultrasound reconciliation → documentation).
- Create patient-facing language templates to explain EDD to expectant parents.
- Draft an implementation plan for a state program to standardize dating methods across facilities.