How to Calculate EDD from LMP – Estimate Your Baby’s Due Date
Determining when a baby is likely to arrive is one of the most important steps in prenatal care. Knowing how to calculate edd from lmp (estimated due date from last menstrual period) is essential not only for scheduling clinical visits and screenings but also for planning maternal nutrition, counseling, and delivery care. This comprehensive guide walks through practical calculations, historical context, public health implications, state-level programs, success stories, pitfalls, and future prospects — all written for clinicians, community health workers, policymakers, and expectant parents.
What is EDD and why does it matter?
The estimated due date (EDD) is a single date used by health providers to guide pregnancy management. It is central to timing prenatal tests, monitoring fetal growth, arranging referrals, and coordinating delivery plans. Learning how to calculate edd from lmp empowers a pregnant person to understand their pregnancy timeline and ensures health systems can provide timely, evidence-based services.
Knowing the EDD affects:
- Timing of first-trimester screening and dating ultrasound.
- Scheduling gestational diabetes testing, anatomy ultrasound, and group B streptococcus screening.
- Decisions about induction, referral for high-risk care, and planning for childbirth in resource-limited settings.
- Enrollment in maternal health programs, financial and social support tied to gestational age, and communication of expected timelines to families.
A brief history: How dating pregnancy evolved
Historically, pregnancy dating relied on maternal recollection, clinical examination, and pattern recognition. The concept of calculating EDD from LMP became standardized with simple rules used by midwives and clinicians. Over time, the practice was formalized into obstetric rules and supplemented by ultrasound dating:
- Early midwifery: Long before modern obstetrics, skilled birth attendants used menstrual history, quickening (fetal movement), and uterine size to estimate term.
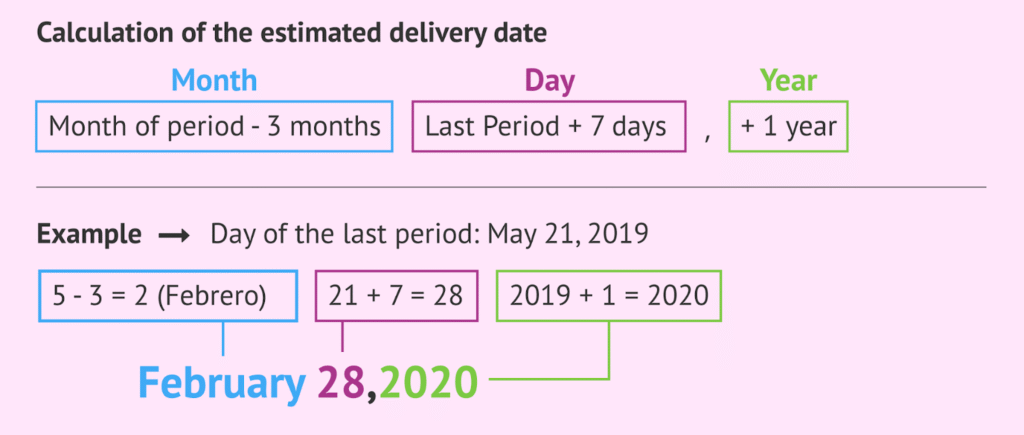
- Naegele’s Rule: In the 19th century, Naegele’s Rule (add one year, subtract three months, add seven days to LMP) became widely adopted in Western medicine as a straightforward method to approximate the EDD.
- Ultrasound era: Since mid-20th century, sonographic crown-rump length in the first trimester improved accuracy, prompting algorithms that reconcile LMP and ultrasound.
- Integration into public health: As maternal and child health programs expanded globally, simple, reliable, and teachable methods for how to calculate edd from lmp became core training for community health workers.
Understanding this historical arc clarifies why simple rules still matter: in many settings, ultrasound is unavailable, so calculating EDD from LMP remains a frontline skill.
The biology behind LMP-based dating
The LMP method assumes a 28-day menstrual cycle with ovulation on day 14. The gestational age (age of the embryo/fetus) is calculated from the first day of the last menstrual period — not from conception — because LMP is easier to recall and standardized in records.
Key points:
- Gestational age by LMP counts from LMP day 0. Conception typically occurs ~14 days after LMP for a textbook 28-day cycle.
- Fertilization and implantation occur after the date counted by LMP; therefore, gestational age is ~2 weeks older than embryonic age.
- Variability in cycle length, irregular cycles, and uncertain recall are the main sources of error in LMP-based dating.
Given biological variability, understanding how to calculate edd from lmp is not just arithmetic; it’s about interpreting that arithmetic within an individual’s menstrual rhythm and access to confirmation tests.
Simple rule: Naegele’s Rule — how to calculate EDD from LMP in practice
Naegele’s Rule is the most commonly taught method for clinicians and laypeople when calculating EDD from LMP. It is simple, reproducible, and requires only the calendar date of the LMP.
To apply Naegele’s Rule:
- Start with the first day of the last menstrual period (LMP).
- Add one year.
- Subtract three months.
- Add seven days.
Example: If LMP is March 10, 2025:
- Add one year → March 10, 2026.
- Subtract three months → December 10, 2025.
- Add seven days → December 17, 2025.
Thus, the EDD is December 17, 2025.
Because many people do mental math on phones or in clinic notes, memorizing this simple algorithm answers most practical questions about how to calculate edd from lmp quickly and reliably.
Variations and quick alternatives
Other common methods and aides include:
- Add 280 days (40 weeks) to the first day of LMP. This is equivalent to Naegele’s Rule and is useful for electronic medical records that add days.
- Count 40 weeks from LMP on a calendar app or use a pregnancy wheel/gestational calculator.
- Smartphone pregnancy calculators: Many apps accept LMP and compute EDD and gestational milestones.
All of these are methods to answer the single core question: how to calculate edd from lmp and convert that date into management steps.
When LMP-based EDD is less accurate
Several situations make LMP-based EDD less reliable:
- Irregular cycles or ovulation later than day 14.
- Recent discontinuation of hormonal contraception or breastfeeding, which alters cycle regularity.
- Uncertain recall of the first day of LMP.
- Conception following assisted reproductive technologies (IVF), where embryo transfer dates are more precise.
In such cases, reconciliation with first-trimester ultrasound dating ensures better accuracy. Still, knowing how to calculate edd from lmp remains useful as an initial step and for triage in low-resource settings.
Ultrasound vs. LMP: reconciling the dates
Ultrasound, particularly crown-rump length in the first trimester, is the gold standard for dating a pregnancy when performed early. When LMP and ultrasound give differing EDDs, clinicians generally follow these principles:
- If the ultrasound dating is within a certain tolerance (e.g., +/- 7 days in the first trimester), LMP is acceptable.
- If ultrasound differs by more than the tolerance, ultrasound dating typically overrides LMP.
Still, providers document both dates and note discrepancies. Understanding how to calculate edd from lmp helps interpret the magnitude and implications of any difference between LMP and ultrasound.
Implementing LMP-based dating in clinics and communities
Training frontline workers in how to calculate edd from lmp is straightforward and high-yield. Implementation steps include:
- Teach Naegele’s Rule and the 280-day addition method.
- Use pregnancy wheels or smartphone calculators to reduce arithmetic errors.
- Encourage documentation of certainty level (exact, approximate, unknown).
- Link the EDD to a timeline of interventions (first antenatal visit, screening tests, iron supplementation, tetanus immunization, referral thresholds).
In rural or resource-constrained settings, LMP-based dating enables earlier, more organized maternal care and better linkage to social services.
Public health objectives tied to accurate dating
Accurately documenting EDD supports several policy goals:
- Timely access to antenatal testing and interventions that reduce maternal and neonatal morbidity.
- Correct capture of gestational age in vital records for surveillance and planning.
- Fair allocation of state-level maternal benefits and entitlements linked to trimester or delivery timing.
- Monitoring of program performance for initiatives that aim to reduce preterm birth and stillbirth.
Knowing how to calculate edd from lmp improves both individual care and aggregated program metrics.
State-wise impact: examples from maternal health programs
Different states and regions implement maternal health programs that rely on gestational age for eligibility and timing. Examples of how LMP-based dating plays a role:
- Enrollment into conditional cash transfer programs may require proof of pregnancy and estimated delivery date. Teaching beneficiaries how to calculate edd from lmp simplifies enrollment and reduces delays.
- State antenatal care schedules are often structured by trimester milestones. Community health workers use LMP calculations to plan home visits, micronutrient supplementation, and counseling.
- Mobile health (mHealth) initiatives that send gestation-specific messages rely on accurate dating; when ultrasound is unavailable, LMP-based EDD allows automated, timely messaging.
By integrating the simple skill of how to calculate edd from lmp into training and program workflows, states can improve reach and timeliness of maternal services.
Women’s empowerment and community engagement
Educating pregnant persons on how to calculate edd from lmp is an empowerment strategy:
- It fosters agency: expectant parents who know their timeline can make informed choices, plan transport, and arrange childcare.
- It demystifies medical timelines: learning the logic behind dating reduces anxiety and increases trust in health systems.
- It links families to resources: accurate dates enable timely enrollment in women empowerment schemes, nutritional support, and cash transfers.
Integrating EDD education into women’s groups and antenatal classes supports broader empowerment objectives.
Rural development and social welfare initiatives
In rural environments where ultrasound availability is limited, LMP-based dating intersects with development initiatives:
- Social welfare programs that disburse benefits across pregnancy can use LMP-derived EDD to schedule support.
- Rural health posts that teach how to calculate edd from lmp can better coordinate outreach clinics and ensure essential medicines are available when needed.
- Linkages between agricultural extension, community nutrition, and maternal health programs rely on predictable gestational timelines to target interventions such as supplementary feeding in late pregnancy.
Thus, simple knowledge of how to calculate edd from lmp supports integrated rural development goals.
Success stories: programs that benefitted from LMP-based dating
Several programmatic examples highlight the value of embedding LMP-based dating into maternal care:
- A district-scale mHealth project trained ASHAs and community volunteers to compute EDD from LMP and enroll pregnant women into a messaging platform; timely reminders improved antenatal visit completion rates and iron supplementation uptake.
- A state-run conditional cash transfer scheme used LMP-derived EDDs to schedule benefit installments. Documenting EDD reduced disputes and ensured payments matched antenatal timelines.
- In regions with limited ultrasound, midwives trained in LMP dating and recognition of red flags were able to triage high-risk pregnancies earlier, reducing emergency transfers and improving outcomes.
Each story reflects how the practical skill of how to calculate edd from lmp translates into measurable health system improvements.
Challenges and limitations
Despite its virtues, LMP-based dating faces challenges:
- Recall bias: Some pregnant people cannot recall LMP accurately, especially with irregular cycles or low health literacy.
- Menstrual irregularities: Polycystic ovary syndrome, recent hormonal contraception, and lactational amenorrhea complicate LMP accuracy.
- Systemic: Health records may be fragmented, with conflicting dates across facilities.
- Equity: Overreliance on ultrasound in urban centers while rural areas depend on LMP can widen disparities if not reconciled.
Addressing these challenges requires both technical fixes (ultrasound access, better record-keeping) and programmatic solutions (training, community outreach) that recognize the practical role of how to calculate edd from lmp.
Comparing schemes and approaches: LMP-based dating within maternal health programs
When comparing maternal health strategies, dating approaches influence outcomes and resource allocation:
- LMP-first approach: Cost-effective, feasible in low-resource settings, but less accurate for irregular cycles.
- Ultrasound-centered approach: Most accurate early in pregnancy, but requires equipment, trained sonographers, and scheduling; may be less accessible in rural areas.
- Hybrid approach: Use LMP for initial planning and confirm with early ultrasound when available; reconcile dates using standardized clinical thresholds.
For policymakers evaluating investments, understanding how to calculate edd from lmp helps in designing equitable, blended approaches that maximize reach while preserving accuracy.
Clinical scenarios and decision-making
Several clinical scenarios illustrate the practical implications of EDD calculations:
- If a pregnant person reports LMP consistent with a 10-week gestation but ultrasound dates at 8 weeks, clinicians may consider ultrasound more reliable and adjust the EDD accordingly.
- When anticipating preterm labor or scheduling a cesarean for obstetric indications, precise dating is critical; if LMP is uncertain, early ultrasound or last-known conception events guide decisions.
- In high-burden settings where timely treatment for conditions like malaria or anemia is linked to gestational age, accurate EDD computation (including how to calculate edd from lmp) supports programmatic triage.
These examples show the downstream clinical importance of a well-documented EDD.
Tools and resources for calculation and documentation
Practical tools that support consistent EDD calculation include:
- Pregnancy wheels used in clinical settings for rapid gesture-based calculation.
- EMR/EHR systems that add 280 days to LMP automatically and link to standardized antenatal checklists.
- Simple charts and wall posters in clinics demonstrating how to calculate edd from lmp for staff and patients.
- Mobile apps and SMS services that accept LMP and return EDD and milestone reminders.
Adoption of these aids reduces calculation errors and standardizes care across providers.
Training healthcare workers: curriculum tips
Training should emphasize:
- The biological underpinning: meaning of gestational age versus fetal age.
- Performing Naegele’s Rule and the 280-day addition method accurately.
- Assessing the certainty of LMP and documenting any uncertainty.
- Reconciling LMP with ultrasound findings using clinical thresholds.
- Communicating the EDD and its uncertainties compassionately to pregnant persons.
A short simulation exercise in which trainees calculate EDD for diverse LMP dates — including irregular cycles — solidifies competence in how to calculate edd from lmp.
Data systems and monitoring
Accurate EDDs feed into monitoring and evaluation:
- Aggregate gestational age distributions inform preterm birth surveillance.
- Program coverage metrics (first antenatal visit before 12 weeks, completion of all antenatal visits) depend on reliable dating.
- State and national reporting on maternal and neonatal indicators uses EDD-aligned denominators for meaningful comparisons.
Thus, standardizing how to calculate edd from lmp supports both clinical care and public health measurement.
Ethical and communication considerations
When communicating EDD:
- Emphasize uncertainty: EDD is an estimate, not a promise.
- Use plain language: explain weeks and months plainly to avoid confusion.
- Respect cultural beliefs: birth narratives and community practices shape perceptions of due dates.
- Avoid deterministic language that can alarm families if dates shift with ultrasound.
Good communication builds trust and reduces the stress associated with variability in EDD derived from how to calculate edd from lmp versus imaging.
Cost-effectiveness and equity
From a systems perspective:
- LMP-based dating is low-cost and scalable, making it appropriate as a baseline strategy for universal prenatal coverage.
- Investing in early ultrasound capacity improves accuracy but requires targeted deployment to avoid exacerbating urban-rural inequities.
- Policies should blend LMP-based systems with strategic ultrasound access, ensuring vulnerable populations benefit from both affordability and precision.
Sound investment strategies recognize the complementary nature of how to calculate edd from lmp and imaging-based dating.
Future prospects: digital tools, AI, and integration
Emerging technologies will influence how EDD is determined and used:
- Smartphone apps with built-in calculators and patient education reduce errors and let patients track milestones derived from how to calculate edd from lmp.
- AI systems could reconcile LMP, wearable fertility data, and early ultrasound to produce probabilistic due date ranges rather than single-point estimates.
- Integration with social support platforms may automatically enroll pregnant people into benefits and reminders timed by EDD, improving uptake of maternal services.
These developments will expand the utility of EDD while preserving the practical role of LMP-based calculations.
Practical checklist: What to document when calculating EDD from LMP
When recording EDD from LMP, note:
- Date of the first day of LMP and whether the date is exact or estimated.
- Method used (Naegele’s Rule, 280-day add).
- Presence and result of early ultrasound dating, if available.
- Any relevant factors (irregular cycles, recent contraceptive use) that affect accuracy.
- Patient counseling notes about uncertainty and expected follow-up.
This simple documentation improves continuity of care and program monitoring.
Integrating EDD education into antenatal care packages
Antenatal care should include a brief module on EDD:
- Teach pregnant people and families how to calculate edd from lmp as part of early visits.
- Provide printed or digital EDD cards with key milestone dates.
- Use EDD to schedule follow-up visits and to explain the importance of timely screening.
Embedding this skill into routine care fosters shared understanding and better outcomes.
Case studies: illustrative vignettes
Case 1: Rural ASHA and timely immunization
An ASHA trained to compute EDD from LMP identified women at 28 weeks for iron and tetanus campaigns. Timely delivery of supplements improved hemoglobin trends in the district.
Case 2: Urban clinic reconciling LMP and ultrasound
A woman with irregular cycles presented with uncertain LMP. Early ultrasound established dating; documented EDD helped plan appropriate screening and prevented unnecessary induction.
Each vignette underscores the intertwined clinical and programmatic benefits of mastering how to calculate edd from lmp.
Challenges to scale and how to overcome them
Scaling training and adoption faces barriers:
- Limited staff time for training — solution: integrate short microlearning modules into routine staff meetings.
- Variable literacy among pregnant people — solution: use pictorial aids and verbal counseling to teach EDD concepts.
- Fragmented records — solution: standardize forms and use electronic registries where feasible.
Addressing these hurdles strengthens the reliability of LMP-based dating across systems.
Recommendations for policymakers and program designers
Policymakers should:
- Standardize documentation formats for LMP and EDD across public health facilities.
- Invest modestly in early ultrasound centers while ensuring LMP-based methods are taught universally.
- Link EDD to program eligibility and ensure mechanisms for updating EDD when ultrasound differs.
- Support community education campaigns that teach simple EDD calculation and promote early antenatal booking.
These steps help align clinical accuracy with broad public health coverage.
Conclusion
Understanding how to calculate edd from lmp is a fundamental, high-return clinical and public health skill. It supports timely antenatal care, links pregnant people to services, and provides a foundation for equitable maternal health programming. While ultrasound improves accuracy, LMP-based methods remain essential, especially where resources are limited. Training, documentation, and integrated systems that recognize both the strengths and limits of LMP-based dating will yield the best outcomes for mothers, babies, and communities.
Frequently Asked Questions
What is the easiest way to calculate EDD from LMP?
- The easiest methods are Naegele’s Rule (add one year, subtract three months, add seven days to the first day of LMP) or simply adding 280 days (40 weeks) to the LMP date. Both give the same result and are widely used in clinical practice.
How accurate is EDD calculated from LMP?
- Accuracy varies. For people with regular 28-day cycles, LMP can be reasonably accurate. However, irregular cycles, uncertain recall, or fertility treatments reduce accuracy. Early first-trimester ultrasound is more precise and is used to confirm or adjust LMP-based EDD.
If ultrasound and LMP give different EDDs, which should I trust?
- In clinical practice, early ultrasound dating often overrides LMP when the discrepancy exceeds accepted tolerance thresholds (commonly ±7 days in the first trimester). Clinicians document both dates and communicate any adjustment clearly to the patient.
Can I calculate EDD from LMP if I have irregular cycles?
- You can still calculate an EDD from LMP, but its reliability is lower. Health workers should note uncertainty and, where possible, arrange early ultrasound or use other markers (e.g., known ovulation dates, prior cycle patterns) to refine dating.
Why is EDD counted from LMP and not conception?
- LMP is used because it is more reliably recalled and standardizes gestational age counting. Conception dates are often uncertain; using LMP provides a consistent reference point across clinical records and research.
How does knowing the EDD help with maternal benefits and social services?
- Many state and national programs schedule benefits and interventions by trimester or specific gestational weeks. An accurately recorded EDD enables timely enrollment, targeted services (e.g., nutrition support), and appropriate scheduling of medical tests and immunizations.
What should I do if I’m unsure of my LMP?
- Tell your healthcare provider as soon as possible. They may offer early ultrasound for dating or use clinical signs to estimate gestational age and monitor pregnancy progression. Meanwhile, expectant parents can still use typical EDD calculators with the best available date and update records when more precise information becomes available.