Pregnancy Due Date Calculator
Calculate your estimated due date (EDD) based on your last period or conception date
Your Pregnancy Due Date
Pregnancy Timeline
Understanding when your baby will arrive can be one of the most meaningful — and anxiety-reducing — moments of pregnancy. The EDD pregnancy calculator is a simple tool that translates key clinical dates into an estimated due date (EDD), helping expectant parents, clinicians, and health programs plan care, resources, and interventions.
In this comprehensive article we’ll explain what an EDD pregnancy calculator is, its history and objectives, how it’s implemented in clinical and public-health contexts, state-level and regional impact, success stories, limitations and challenges, comparisons with alternative methods, and prospects for future development. Along the way we’ll integrate policy framework considerations, state-wise benefits, women empowerment schemes, rural development, and social welfare initiatives that leverage accurate pregnancy dating to improve maternal and neonatal outcomes.
What is an EDD pregnancy calculator?
An EDD pregnancy calculator estimates the Expected Date of Delivery — the probable date when labor might start — based on known pregnancy milestones. Clinicians and expectant parents commonly use either the first day of the last menstrual period (LMP) or the date of conception/assisted reproductive treatment to calculate the due date. Modern EDD pregnancy calculators may also incorporate ultrasound measurements like crown–rump length (CRL) or biparietal diameter (BPD) to refine dating, especially when LMP is uncertain.
Accurate use of an EDD pregnancy calculator helps determine gestational age, schedule prenatal appointments, time diagnostic tests (for example, glucose tolerance test or anomaly scan), and prepare for delivery logistics. Beyond individual care, aggregated EDD data can inform program planning, supply chain forecasting (e.g., for iron, oxytocin, neonatal equipment), and public-health policy.
Brief history and evolution of pregnancy dating
Pregnancy dating has evolved from simple folklore and observational methods to standardized clinical practice. Historically, communities estimated childbirth timing through observable signs and traditional calendars. The formalization of the expected due date began in the 19th century when clinicians recognized the link between menstrual cycles and fetal development. Naegele’s rule — adding seven days to the first day of the last menstrual period and subtracting three months — became a widespread heuristic for calculating due dates.
As obstetric ultrasound became available in the mid-20th century, medical practitioners began to refine dates with biometric measures. The modern EDD pregnancy calculator now combines rules-based approaches like Naegele’s rule with biometric data and algorithmic adjustments for cycle length, conception dates, and ART (assisted reproductive technology) timing. Digital calculators and smartphone apps have made EDD pregnancy calculators instantly accessible to millions worldwide, increasing awareness and allowing cross-checks between patient and provider estimates.
Objectives of using an EDD pregnancy calculator
The primary objectives of an EDD pregnancy calculator include:
- Establishing gestational age to guide prenatal screening and interventions.
- Scheduling key prenatal tests and vaccinations at appropriate windows.
- Planning for maternal and newborn care resources at health facilities.
- Improving perinatal surveillance, timely referrals, and emergency preparedness.
- Empowering expectant parents with knowledge that reduces anxiety and improves adherence to care plans.
From a public-health and policy perspective, accurate EDD estimation supports program monitoring (e.g., tracking antenatal coverage by gestational age), resource allocation in state-wise benefits programs, and data-driven interventions in women empowerment schemes and rural development initiatives.
How the EDD pregnancy calculator works — methods and inputs
There are several approaches an EDD pregnancy calculator may use, and each has advantages and limits. The main methods are:
- LMP-based calculation (Naegele’s rule)
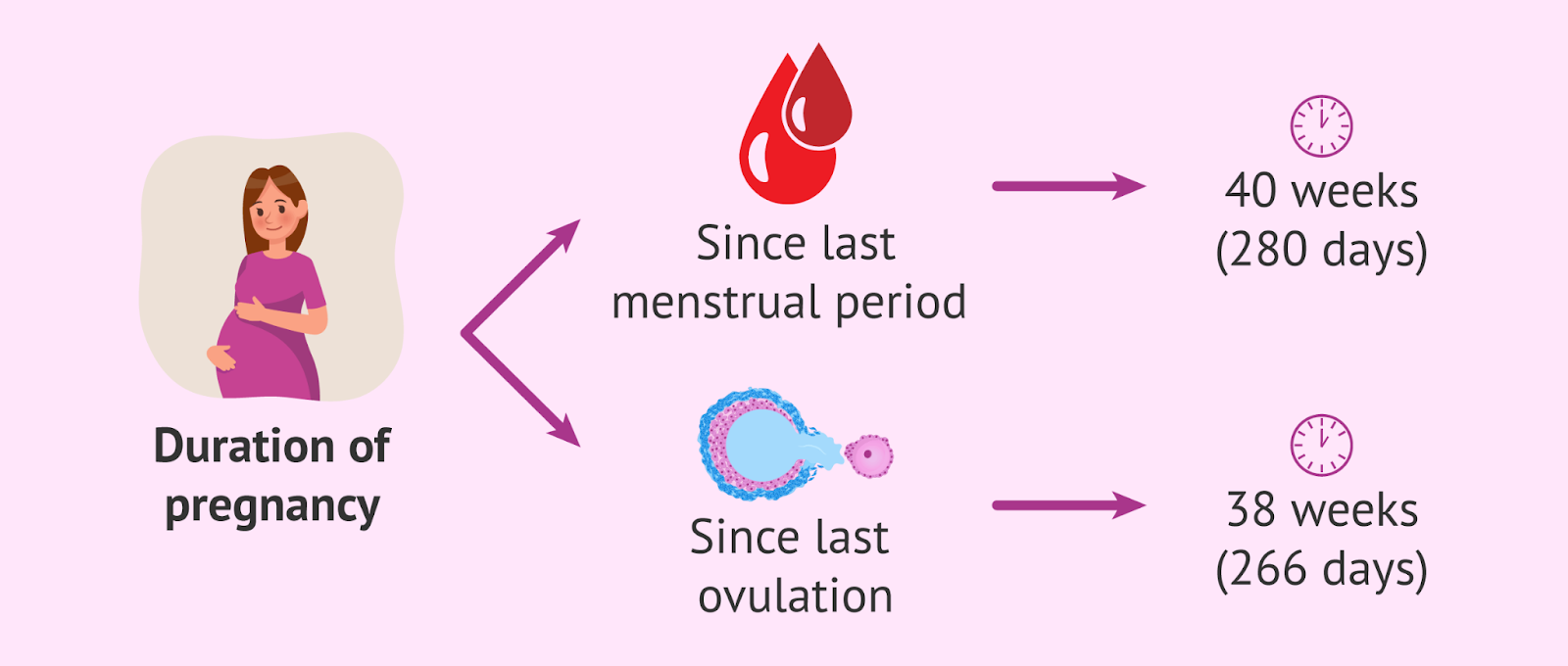
This common method requires the first day of the last menstrual period. Using Naegele’s rule, the calculator adds 280 days (40 weeks) to that date. Adjustments are often made for abnormal cycle lengths. - Conception-date calculation
If conception date is known (for example, through ovulation tracking or timing of intercourse), the calculator adds 266 days (38 weeks) from conception. This method can be more accurate when LMP is unreliable. - Ultrasound-based dating
Early pregnancy ultrasound is the most accurate method for dating when performed in the first trimester. Measurements such as crown–rump length are converted into gestational age using standardized growth charts; the EDD is derived accordingly. Ultrasound-based EDD is preferred when LMP is uncertain or cycles are irregular. - Embryo transfer or ART-based dating
For pregnancies conceived via IVF or intrauterine insemination, the date of embryo transfer or insemination provides precise dating input; the calculator uses that date to estimate EDD. - Hybrid algorithms
Many modern EDD pregnancy calculators combine inputs: LMP, ultrasound, cycle length, and clinical judgment. Some clinical information systems apply hierarchies — for example, prioritizing early ultrasound estimates over LMP when discrepancies occur.
Clinical implementation and best practices
Healthcare providers rely on validated processes to integrate an EDD pregnancy calculator into prenatal care:
- First prenatal visit: Record detailed menstrual history, any fertility treatments, and perform early ultrasound when indicated. Enter these data into the EDD pregnancy calculator.
- Prioritization rules: Adopt institutional rules for reconciling multiple dating methods: often ultrasound in the first trimester supersedes LMP if discrepancy exceeds a clinically meaningful threshold (e.g., >7 days for first-trimester ultrasound).
- Documentation: Clearly document the chosen EDD and the method used. This avoids confusion during subsequent visits and in handoffs between providers or facilities.
- Patient education: Explain how the EDD was calculated and emphasize that it is an estimate, not a guaranteed delivery date. Discuss the range of normal variation (generally ±2 weeks around term).
- Integration with scheduling: Use the EDD to schedule appropriate tests (e.g., anatomy scan at 18–22 weeks), vaccinations (e.g., tetanus, influenza), and counseling sessions (e.g., birth preparedness, breastfeeding).
Clinicians who standardize use of an EDD pregnancy calculator reduce errors, align patient expectations, and improve quality metrics such as timely antenatal visits and screening uptake.
State-wise implementation and regional impact
At the systems level, many public-health programs incorporate EDD tracking into maternal health registries, digital health platforms, and antenatal care registers. Accurate EDD information supports:
- Resource allocation: Predicting delivery load at district hospitals and primary health centers allows health departments to deploy staff, medicines, and equipment to meet demand.
- Supply chain planning: Forecasting needs for uterotonics, oxytocin, clean delivery kits, and neonatal resuscitation can be aligned to expected deliveries derived from aggregated EDD data.
- Referral systems: Identifying pregnancies approaching term that require institution-based delivery or special care helps prioritize referral transport and facility readiness.
- Program evaluation: State-wise benefits and women empowerment schemes (for example, conditional cash transfers for institutional delivery) can monitor whether incentives are claimed in the anticipated time windows.
Regional impact depends on infrastructure: states with robust digital health records and high antenatal coverage gain substantial efficiency from systematic use of an EDD pregnancy calculator. In contrast, areas with low antenatal attendance or limited ultrasound access must focus on strengthening front-line services to capture reliable dating data.
EDD pregnancy calculator and women’s empowerment schemes
Integrating the EDD pregnancy calculator into women empowerment schemes magnifies benefits:
- Conditional benefits: Programs that provide cash incentives for institutional delivery, antenatal visit completion, or immunization adherence can use EDD data to define eligibility windows and verify compliance.
- Targeted outreach: Health workers can use EDD lists to prioritize home visits, counsel women on birth preparedness, and connect pregnant women to social support services.
- Education and autonomy: When women understand their gestational timeline through an accessible EDD pregnancy calculator, they are better able to make informed decisions about delivery location, family planning, and newborn care.
- Monitoring and accountability: EDD-based reporting provides measurable indicators for program performance, improving transparency and accountability in social welfare initiatives.
When combined with respectful, culturally sensitive care, EDD-informed programming supports both clinical outcomes and empowerment goals.
The role of EDD pregnancy calculators in rural development and social welfare
Rural populations often face access constraints to timely prenatal care. An EDD pregnancy calculator embedded within community health platforms or mobile health (mHealth) programs can:
- Help community health workers prioritize visits before and around the EDD.
- Aid in arranging transportation and facility-based delivery for remote women with expected high-risk pregnancies.
- Inform community-level planning for childbirth preparedness, including local birth attendants and referral communication.
- Feed data into social welfare initiatives for targeted support (nutritional supplementation, maternity entitlements) timed to gestation.
By linking EDD data to rural development strategies, local governments can better integrate maternal health priorities into broader development planning — from road improvements for emergency transport to village-level awareness campaigns.
Success stories: tangible benefits of accurate EDD tracking
Several health programs and facilities have reported measurable improvements after incorporating accurate due-date estimation:
- Improved scheduling of antenatal tests: Facilities using EDD calculators reported higher rates of on-time anomaly scans and screening tests, enabling earlier detection of fetal anomalies or maternal complications.
- Better maternal referral outcomes: Districts that used EDD registries to coordinate transport for women nearing term had lower rates of last-minute emergency transfers and improved maternal satisfaction.
- Efficient resource utilization: Hospitals that forecasted delivery caseloads based on aggregated EDDs optimized staffing patterns and lowered overtime costs without sacrificing quality.
- Increased uptake of institutional deliveries: Incentive programs tied to EDD timelines saw higher claims and improved institutional delivery rates when due dates were systematically tracked and communicated to beneficiaries.
These success stories illustrate how an EDD pregnancy calculator fosters clinical precision and administrative effectiveness.
Common challenges and limitations
Despite clear benefits, several challenges complicate the use of an EDD pregnancy calculator:
- Unreliable LMP: Irregular cycles, poor recall, or amenorrhea can make LMP-based estimates inaccurate.
- Late antenatal presentation: When women first present after the first trimester, ultrasound dating is less precise, and the EDD estimate widens.
- Access to ultrasound: Resource-poor settings may lack early ultrasound services, reducing dating accuracy.
- Variability in algorithms: Different calculators and institutions may apply different rules for reconciling LMP and ultrasound, producing inconsistent EDDs.
- Patient misunderstanding: Misinterpreting EDD as a fixed appointment rather than an estimate can lead to disappointment or poor planning.
- Data quality and interoperability: Incomplete or fragmented records across facilities undermine the utility of aggregated EDD data for program planning.
Addressing these limitations requires combined investments in training, equipment, digital records, and patient education.
Clinical comparison: EDD pregnancy calculator versus alternative dating methods
Comparing common approaches highlights trade-offs:
- LMP (Naegele’s rule): Readily available and low-cost but sensitive to recall bias and cycle irregularity.
- Ultrasound dating: More accurate in the first trimester; precision declines later in pregnancy. Requires equipment and trained personnel.
- Conception/ART-based dating: Very precise for assisted conceptions but unavailable for spontaneous pregnancies without reliable conception timing.
- Biomarkers and emerging techniques: Research explores biochemical markers and AI models for gestational age estimation, but these are not yet standard clinical practice.
An integrated approach — using the most reliable available input, prioritizing early ultrasound when possible, and clarifying the method used — provides the best balance between accuracy and feasibility.
Technology trends: digital EDD pregnancy calculators and mHealth
Digital health solutions have expanded access to EDD calculation:
- Mobile apps: Many apps provide EDD pregnancy calculators for personal use, tracking symptoms, appointment reminders, and educational content. While convenient, app accuracy depends on input quality and algorithm transparency.
- Electronic medical records (EMR): Clinical EMRs can standardize EDD calculation rules and automatically schedule tests and alerts based on the estimated date.
- mHealth for community workers: Simple tools allow frontline providers to enter LMP or ultrasound dates and generate EDD lists for outreach and referral planning.
- AI and prediction models: Research is exploring predictive models that incorporate demographic, biometric, and biochemical data to refine gestational age estimates, but clinical validation and ethical oversight are necessary before widespread adoption.
When properly governed and validated, technology-enabled EDD pregnancy calculators can scale benefits while maintaining data security and clinical reliability.
Ethical and policy considerations
Implementing EDD-based systems at scale raises important ethical and policy questions:
- Equity: Ensuring underserved populations (rural, low-income, marginalized groups) have access to reliable dating services avoids widening disparities.
- Informed consent and data privacy: Collecting and using EDD data must follow privacy norms and secure data practices, particularly when aggregated for program planning.
- Transparency of algorithms: Tools should disclose how EDDs are calculated and any limitations to avoid misinformation.
- Integration with benefits: Linking EDDs to social benefits requires safeguards against misuse or fraud while maximizing benefit to eligible mothers.
- Training and accountability: Policymakers should mandate clinician training on dating rules and standardization to minimize variation and errors.
A policy framework that centers equity, privacy, and quality will amplify the positive impact of EDD systems.
Measuring impact: indicators and monitoring
Programs using an EDD pregnancy calculator should track indicators that reflect both clinical and administrative outcomes:
- Proportion of pregnancies with documented EDD and dating method.
- Percentage of pregnancies with first-trimester ultrasound dating.
- Timeliness of key antenatal interventions relative to gestational windows.
- Institutional delivery rates and referral timeliness for high-risk pregnancies.
- Supply stockouts or resource mismatches reduced by EDD-based forecasting.
- Beneficiary satisfaction and awareness of expected delivery timelines.
Monitoring these indicators helps programs iterate and strengthen maternal and newborn services.
Implementation roadmap for health systems
Health systems aiming to harness the EDD pregnancy calculator effectively can consider a phased approach:
- Standards and protocols: Define national or state rules for reconciling LMP and ultrasound dating, and publish clear documentation for providers.
- Capacity building: Train clinicians and community health workers on dating methods, documentation, and patient communication.
- Equipment and access: Expand access to early ultrasound where feasible and integrate low-cost portable devices in underserved areas.
- Digital integration: Add EDD calculators and scheduling functionality to EMRs and community health apps with built-in privacy protections.
- Community engagement: Educate expectant parents about what EDD means and how to use the information for birth planning.
- Evaluation and feedback: Continually measure outcomes and refine processes to reduce discrepancies and optimize resource use.
A pragmatic roadmap ensures sustainable integration of the EDD pregnancy calculator into routine care.
Case studies: how EDD data improved outcomes
Consider hypothetical but plausible case vignettes illustrating impact:
- In a semi-urban district, the health department used aggregated EDDs to forecast monthly delivery volumes at primary facilities. This allowed staff reallocation, reducing overcrowding and improving postpartum monitoring. Institutional delivery rates rose and patient-reported satisfaction improved after EDD-driven scheduling.
- A rural maternal health program trained community health workers to use a simple EDD pregnancy calculator on mobile phones. The workers prioritized home visits to women within two weeks of their EDD, ensuring clean delivery plans and emergency transport arrangements. Neonatal complication rates decreased as a result of timely referral.
- A state-run women empowerment scheme linked antenatal cash transfers to EDD milestones to verify attendance at critical visits. By comparing EDDs recorded in clinic registers with program claims, administrators tightened program targeting while maintaining timely support for beneficiaries.
Each example underscores how pragmatic use of EDD information translates into better planning and outcomes.
Addressing skepticism: common myths about EDD
Several misconceptions about the EDD pregnancy calculator persist:
- Myth: EDD is exact — In reality, an EDD is an estimate. Most births occur within a window around the due date; clinicians view term as 37 to 42 weeks.
- Myth: A late ultrasound is just as accurate — Early ultrasounds are most reliable; accuracy decreases as gestation advances.
- Myth: EDD eliminates uncertainty — While helpful for planning, EDD cannot predict the exact day of labor onset nor all obstetric complications.
- Myth: Different calculators give wildly different results — With standardized inputs and reconciliation rules, variation can be minimized; disagreements should be resolved using best-practice prioritization.
Clarifying these points helps pregnant persons and families use EDD information constructively.
Future prospects and innovations
The future of the EDD pregnancy calculator is promising, with several likely trajectories:
- Wider adoption of validated mobile tools: Low-cost apps integrated with national health systems will empower families and providers, especially in remote areas.
- Improved interoperability: Standardized data formats for EDDs will enable seamless transfer between facilities and programs, enhancing continuity of care.
- AI-enhanced models: Machine learning may improve gestational age estimates by integrating multiple data types, but careful validation and transparency will be vital.
- Telemedicine integration: Remote consultations can use EDDs to prioritize care and support home-based monitoring when appropriate.
- Policy-driven scale-up: State-wise programs that tie maternal benefits to documented EDDs will propose efficiencies, but must guard against perverse incentives.
As technology advances, the central challenge will be ensuring equity, validation, and alignment with patient-centered care.
Practical tips for expectant parents using an EDD pregnancy calculator
Expectant parents can use an EDD pregnancy calculator effectively by following practical steps:
- Keep accurate records of your LMP or any dates related to conception or fertility treatments and share these with your provider.
- Ask for early ultrasound dating if menstrual dates are uncertain.
- Understand that the EDD is an estimate; prepare for a range of possible delivery dates rather than a single fixed day.
- Use the EDD to schedule prenatal appointments, pack a delivery bag in advance, and organize transport plans.
- Communicate your EDD to family and caregivers so they can support you around the expected timeframe.
These steps help translate EDD information into actionable birth preparedness.
Recommendations for policymakers and program managers
Policymakers and program managers can maximize the value of an EDD pregnancy calculator by:
- Standardizing dating protocols across public facilities and training staff accordingly.
- Investing in early ultrasound capacity and ensuring equitable access in rural areas.
- Integrating EDD fields in digital health registries and making aggregated EDD data available for planning while preserving privacy.
- Linking EDD-based forecasting to logistics planning and women empowerment schemes, ensuring benefits align with gestational timelines.
- Monitoring outcomes and conducting research on local dating accuracy to iterate policy decisions.
Thoughtful policy choices will enable EDD systems to support both clinical care and broader social initiatives.
Conclusion
The EDD pregnancy calculator is more than a simple arithmetic tool. It is a clinical and programmatic linchpin that supports personalized prenatal care, strengthens health-system planning, and amplifies the impact of social welfare and women empowerment initiatives. Accurate pregnancy dating — whether derived from LMP, early ultrasound, conception dates, or hybrid algorithms — enables timely screening, resource forecasting, and targeted outreach, especially when integrated into state-wise benefits and rural development programs.
While challenges remain — including access inequities, documentation gaps, and algorithm variability — the strategic use of EDD data promises measurable improvements in maternal and neonatal outcomes. As digital health, portable ultrasound, and data-driven planning spread, the EDD pregnancy calculator will remain a vital instrument in the pursuit of safer pregnancies and stronger communities.